Manejo del abdomen abierto en el paciente crítico en un centro de nivel III de Popayán
DOI:
https://doi.org/10.30944/20117582.847Palabras clave:
técnicas de abdomen abierto, control de daños, heridas y traumatismos, infecciones, urgencias médicas, complicaciones posoperatoriasResumen
Introducción. El abdomen abierto es un recurso útil para el tratamiento de pacientes con patología abdominal compleja, con potencial de complicaciones. El objetivo de este estudio fue adaptar la guía de World Society of Emergency Surgery (WSES) 2018, en un hospital de nivel III de atención de la ciudad de Popayán, Colombia, y comparar los resultados obtenidos con los previos a su implementación.
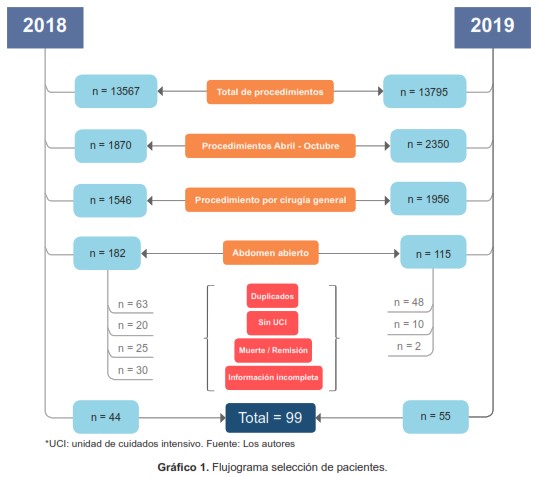
Métodos. Estudio cuasi-experimental en dos mediciones de pacientes con abdomen abierto y estancia en cuidado crítico, durante los meses de abril a octubre de los años 2018 y 2019, antes y después de la adaptación con el personal asistencial de la guía de práctica clínica WSES 2018. Se utilizó estadística descriptiva, prueba de Chi cuadrado y se empleó el software SPSS V.25.
Resultados. Se incluyeron 99 pacientes críticos, con una edad media de 53,2 años, con indicación de abdomen abierto por etiología traumática en el 28,3 %, infecciosa no traumática en el 32,3 % y no traumática ni infecciosa en el 37,4 %. La mortalidad global fue de 25,3 %, de los cuales, un 68 % se debieron a causas ajenas a la patología abdominal. Las complicaciones postoperatorias se presentaron en 10 pacientes con infección de sitio operatorio y 9 pacientes con fístula enterocutánea. El uso del doble Viaflex se implementó en un 63,6 %, logrando un cierre de la pared abdominal en el 79,8 % de los casos (p=0,038).
Conclusión. El abdomen abierto requiere de un abordaje multidisciplinar. El uso de doble Viaflex es una herramienta simple y efectiva. La implementación de la guía disminuyó el porcentaje de mortalidad, los días de abdomen abierto y la estancia en cuidados intensivos.
Descargas
Referencias bibliográficas
Atema JJ, Gans SL, Boermeester MA. Systematic review and meta-analysis of the open abdomen and temporary abdominal closure techniques in non-trauma patients. World J Surg. 2015;39:912–25. https://doi.org/10.1007/s00268-014-2883-6
Cirocchi R, Birindelli A, Biffl WL, Mutafchiyski V, Popivanov G, Chiara O, et al. What is the effectiveness of the negative pressure wound therapy (NPWT) in patients treated with open abdomen technique? A systematic review and meta-analysis. J Trauma Acute Care Surg. 2016;81:575–84. https://doi.org/10.1097/TA.0000000000001126
Muhammad Y, Gondal KM, Khan UA. Use of the ‘Bogota bag’ for closure of open abdominal wound after exploratory laparotomy − our experience at Mayo Hospital Lahore. J Pak Med Assoc. 2016;66:980–3. https://pubmed.ncbi.nlm.nih.gov/27524532/
Kirshtein B, Roy-Shapira A, Lantsberg L, Mizrahi S. Use of the “Bogota bag” for temporary abdominal closure in patients with secondary peritonitis. Am Surg. 2007;73:249–52. https://doi.org/10.1177/000313480707300310
Coccolini F, Roberts D, Ansaloni L, Ivatury R, Gamberini E, Kluger Y, et al. The open abdomen in trauma and non-trauma patients: WSES guidelines. World J Emerg Surg. 2018;13. https://doi.org/10.1186/s13017-018-0167-4
Launey Y, Duteurtre B, Larmet R, Nesseler N, Tawa A, Mallédant Y, et al. Risk factors for mortality in postoperative peritonitis in critically ill patients. World J Crit Care Med. 2017;6:48–55. https://doi.org/10.5492/wjccm.v6.i1.48
Kreis BE, de Mol van Otterloo AJ, Kreis RW. Open abdomen management: a review of its history and a proposed management algorithm. Med Sci Monit. 2013;19:524–33. https://doi.org/10.12659/MSM.883966
Sharrock AE, Barker T, Yuen HM, Rickard R, Tai N. Management and closure of the open abdomen after damage control laparotomy for trauma. A systematic review and meta-analysis. Injury. 2016;47:296–306. https://doi.org/10.1016/j.injury.2015.09.008
Yandell R, Wang S, Bautz P, Shanks A, O’Connor S, Deane A, et al. A retrospective evaluation of nutrition support in relation to clinical outcomes in critically ill patients with an open abdomen. Aust Crit Care. 2019;32:237– 42. https://doi.org/10.1016/j.aucc.2018.04.004
Kim IB, Prowle J, Baldwin I, Bellomo R. Incidence, risk factors and outcome associations of intra-abdominal hypertension in critically ill patients. Anaesth Intensive Care. 2012;40:79–89. http://doi.org/10.1177/0310057X1204000107
Hecker A, Reichert M, Reuß CJ, Schmoch T, Riedel JG, Schneck E, et al. Intra-abdominal sepsis: new definitions and current clinical standards. Langenbecks Arch Surg. 2019;404:257–71. https://doi.org/10.1007/s00423-019-01752-7
Perez D, Wildi S, Demartines N, Bramkamp M, Koehler C, Clavien PA. Prospective evaluation of vacuum-assisted closure in abdominal compartment syndrome and severe abdominal sepsis. J Am Coll Surg. 2007;205:586–92. https://doi.org/10.1016/j.jamcollsurg.2007.05.015
Hodgson CL, Berney S, Harrold M, Saxena M, Bellomo R. Clinical review: early patient mobilization in the ICU. Crit Care. 2013;17:207. https://doi.org/10.1186/cc11820
Giudicelli G, Rossetti A, Scarpa C, Buchs NC, Hompes R, Guy RJ, et al. Prognostic factors for enteroatmospheric fistula in open abdomen treated with negative pressure wound therapy: A multicentre experience. J Gastrointest Surg. 2017;21:1328–34. https://doi.org/10.1007/s11605-017-3453-7
Harvin JA, Mims MM, Duchesne JC, Cox CS, Wade CE, Holcomb JB, et al. Chasing 100%: The use of hypertonic saline to improve early, primary fascial closure after damage control laparotomy. J Trauma Acute Care Surg. 2013;74:426–32. https://doi.org/10.1097/TA.0b013e31827e2a96
Webb LH, Patel MB, Dortch MJ, Miller RS, Gunter OL, Collier BR. Use of a furosemide drip does not improve earlier primary fascial closure in the open abdomen. J Emerg Trauma Shock. 2012;5:126–9. https://doi.org/10.4103/0974-2700.96480
Reignier J, Boisramé-Helms J, Brisard L, Lascarrou JB, Hssain AA, Anguel N, et al. Enteral versus parenteral early nutrition in ventilated adults with shock: a randomised, controlled, multicentre, open-label, parallel-group study (NUTRIREA-2). Lancet. 2018;391:133–43. https://doi.org/10.1016/S0140-6736(17)32146-3
Goh EL, Chidambaram S, Segaran E, Garnelo-Rey V, Khan MA. A meta-analysis of the outcomes following enteral vs parenteral nutrition in the open abdomen in trauma patients. J Crit Care. 2020;56:42–8. https://doi.org/10.1016/j.jcrc.2019.12.001
Sanchez-Betancourt A, Gonzalez-Cole M, Sibaja P, Fernandez L, Norwood S. Cost evaluation of temporary abdominal closure methods in abdominal sepsis patients successfully treated with an open abdomen. Should we take temporary abdominal closure methods at face value? Health economic evaluation. Ann Med Surg (Lond). 2020;56:11–6. https://doi.org/10.1016/j.amsu.2020.06.007
Sava J, Alam HB, Vercruysse G, Martin M, Brown CVR, Brasel K, et al. Western Trauma Association critical decisions in trauma: Management of the open abdomen after damage control surgery. J Trauma Acute Care Surg. 2019;87:1232–8. https://doi.org/10.1097/TA.0000000000002389
Manterola C, Moraga J, Urrutia S. Laparostomía contenida con bolsa de Bogotá. Resultados de una serie de casos. Cir Esp. 2011;89:379–85. https://doi.org/10.1016/j.ciresp.2011.01.010
Doyon A, Devroede G, Viens D, Saito S, Rioux A, Echavé V, et al. A simple, inexpensive, life-saving way to perform iterative laparotomy in patients with severe intra-abdominal sepsis. Colorectal Dis. 2001;3:115–21. https://doi.org//10.1111/j.1463-1318.2001.00214.x
El Maksoud AWM, Mostafa K, Abdel-latif M, Al Hamadi HAB. Outcome of open abdomen procedure with Bogota bag for temporary abdominal closure: our experience in Alexandria University Hospital. The Egyptian Journal of Surgery. 2019;38:807–13.
Coccolini F, Montori G, Ceresoli M, Catena F, Moore EE, Ivatury R, et al. The role of open abdomen in non-trauma patient: WSES Consensus Paper. World J Emerg Surg. 2017;12:39. https://doi.org/10.1186/s13017-017-0146-1
Chatzicostas C, Roussomoustakaki M, Vlachonikolis IG, Notas G, Mouzas I, Samonakis D, Kouroumalis EA. Comparison of Ranson, APACHE II and APACHE III scoring systems in acute pancreatitis. Pancreas. 2002;25:331–5. https://doi.org/10.1097/00006676-200211000-00002
Poillucci G, Podda M, Russo G, Perri SG, Ipri D, Manetti G, et al. Open abdomen closure methods for severe abdominal sepsis: a retrospective cohort study. Eur J Trauma Emerg Surg. 2020 May 6. Online ahead of print. http://dx.doi.org/10.1007/s00068-020-01379-0
Azuhata T, Kinoshita K, Kawano D, Komatsu T, Sakurai A, Chiba Y, Tanjho K. Time from admission to initiation of surgery for source control is a critical determinant of survival in patients with gastrointestinal perforation with associated septic shock. Crit Care. 2014;18:R87. https://doi.org/10.1186/cc13854
Borraez OA. Abdomen abierto: la herida más desafiante. Rev Colomb Cir. 2008;23:204-9.
Descargas
Publicado
Cómo citar
Número
Sección
Licencia
Derechos de autor 2021 Revista Colombiana de Cirugía

Esta obra está bajo una licencia internacional Creative Commons Atribución-NoComercial-SinDerivadas 4.0.
Todos los textos incluidos en la Revista Colombiana de Cirugía están protegidos por derechos de autor. Las opiniones expresadas en los artículos firmados son las de los autores y no coinciden necesariamente con las de los directores o los editores de la Revista Colombiana de Cirugía. Las sugerencias diagnósticas o terapéuticas como elección de productos, dosificación y métodos de empleo corresponden a la experiencia y al criterio de los autores.















.jpg)